Am Fam Physician. 2015 Jan 15;91(2):86-92.
![]() Patient information: See related handout on wound care, written by the authors of this article.
Patient information: See related handout on wound care, written by the authors of this article.
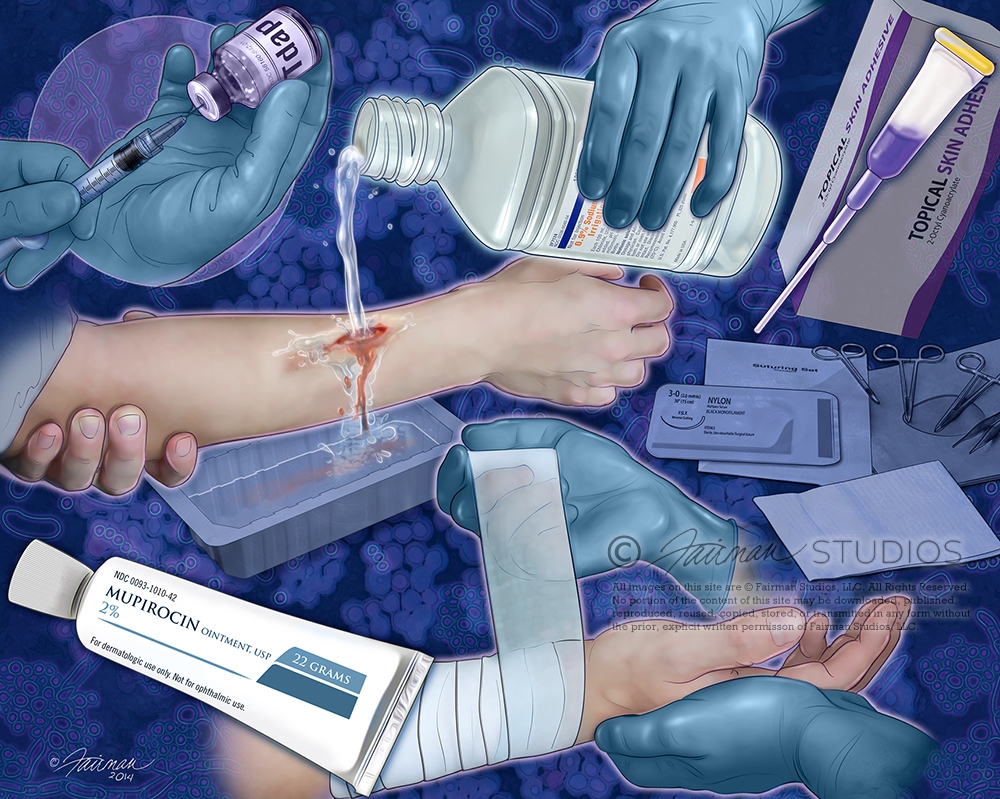
Lacerations, abrasions, burns, and puncture wounds are common in the outpatient setting. Because wounds can quickly become infected, the most important aspect of treating a minor wound is irrigation and cleaning. There is no evidence that antiseptic irrigation is superior to sterile saline or tap water. Occlusion of the wound is key to preventing contamination. Suturing, if required, can be completed up to 24 hours after the trauma occurs, depending on the wound site. Tissue adhesives are equally effective for low-tension wounds with linear edges that can be evenly approximated. Although patients are often instructed to keep their wounds covered and dry after suturing, they can get wet within the first 24 to 48 hours without increasing the risk of infection. There is no evidence that prophylactic antibiotics improve outcomes for most simple wounds. Tetanus toxoid should be administered as soon as possible to patients who have not received a booster in the past 10 years. Superficial mild wound infections can be treated with topical agents, whereas deeper mild and moderate infections should be treated with oral antibiotics. Most severe infections, and moderate infections in high-risk patients, require initial parenteral antibiotics. Severe burns and wounds that cover large areas of the body or involve the face, joints, bone, tendons, or nerves should generally be referred to wound care specialists.
Family physicians often treat patients with minor wounds, such as simple lacerations, abrasions, bites, and burns. This article reviews common questions associated with wound healing and outpatient management of minor wounds. More chronic, complex wounds such as pressure ulcers1 and venous stasis ulcers2 have been addressed in previous articles.